Hair loss is one of those problems that feels deeply personal but is almost universal. For most of us, it creeps in slowly — a little more scalp showing in the mirror, a hairline that’s just slightly higher than last year.
I’ve experienced it myself, and that’s what pushed me to dig into the science behind why hair really falls out — and, more importantly, how to stop it. What began as casual curiosity turned into months of research through studies, medical papers, and first-hand experimentation.
This article ended up being much bigger than I first expected — much like the complexity of hair loss itself. So if you’re serious about getting to the root of it (pun intended), sit down and buckle up. I believe this to be one of the most in-depth articles on the current science of hair loss on the internet, and I will continue to update as it progresses.
There’s no single cause or cure, only layers of biology, hormones, inflammation, and metabolism all working together. My goal here is to unpack all of it in a way that actually makes sense: to explain why hair loss happens, what the latest science says about treatments that genuinely work (and those that don’t), and how to build a realistic, sustainable plan whether you prefer medical, mechanical, or natural approaches.
By the end, you’ll understand the root causes — from DHT and insulin resistance to follicle hypoxia and mitochondrial decline — and how each treatment fits into the bigger picture. Whether you want to go all in with proven medications or stay drug-free with options like microneedling, red-light therapy, or rosemary oil, you’ll walk away knowing exactly what’s worth your time, what’s backed by evidence, and how to combine methods for the best possible results.
The Science of Hair Loss
When people talk about baldness, genetics is often the first thing they blame. Genes do play a role, but they don’t tell the whole story. Look a little deeper, and the next explanation you’ll often hear is “too much testosterone.” That’s not quite right either.
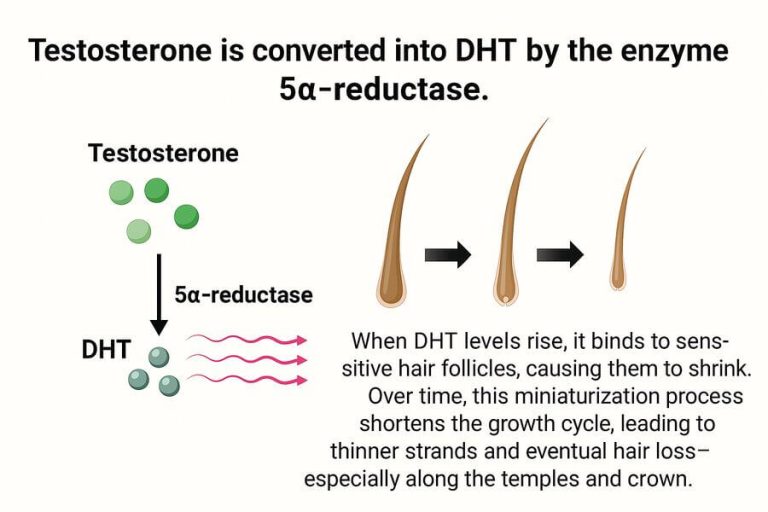
The real culprit behind most cases of hair loss is a condition called androgenetic alopecia (AGA)—commonly known as male or female pattern hair loss. The problem isn’t how much testosterone you have overall, but rather how your hair follicles respond to one of its byproducts: dihydrotestosterone (DHT).
Inside the scalp, an enzyme called 5-alpha-reductase converts testosterone into DHT. Certain follicles—especially those along the temples, hairline, and crown—carry highly sensitive androgen receptors.
These follicles overreact to DHT, and over time they begin to shrink. This process, called miniaturization, shortens the hair growth cycle, producing thinner and weaker hairs with each pass until eventually, no hair grows at all.
But hormones are only part of the picture. Researchers now recognize that hair loss is also shaped by the follicle’s microenvironment. Hair follicles are uniquely demanding structures: they require a high level of oxygen to sustain growth. When blood flow decreases and oxygen levels drop, stress signals build up.
At the same time, the mitochondria—the cell’s energy factories—slow down, leaving hairs without the fuel they need to stay in the growth phase. To make matters worse, inflammation sets in around struggling follicles, and over time this triggers fibrosis, or the buildup of scar-like tissue. That’s why bald patches often look smooth and shiny—the surrounding “soil” has hardened, locking follicles out of action.
While DHT may flip the switch that starts the balding process, inflammation, oxygen loss, and scarring are what keep it permanently stuck in the “off” position. This is why early intervention matters—once a follicle has been choked by fibrosis, waking it back up becomes far more difficult.
Why Patterns Matter (The Norwood Scale)
Hair loss doesn’t strike at random. It follows surprisingly predictable patterns, which is why doctors use the Norwood scale to classify male pattern baldness. This scale runs from a mild temple recession (Norwood 1–2) all the way to extensive loss across the top of the scalp with only a horseshoe of hair remaining (Norwood 7).
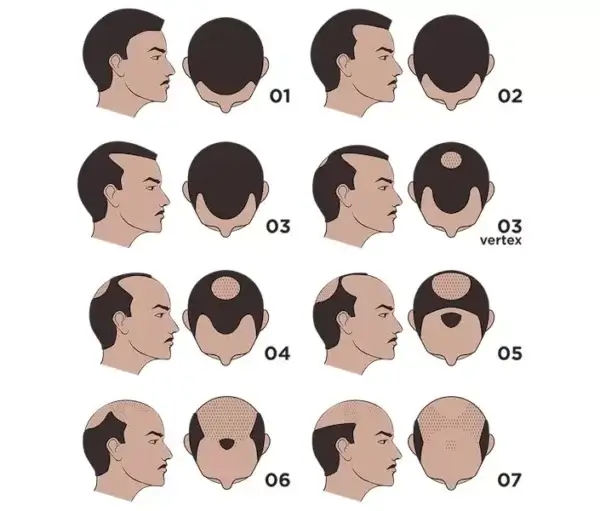
Most men fall into one of two starting patterns. The first begins with frontal recession, where the temples and hairline slowly creep back over the years. The second starts with vertex thinning, where a small bald spot appears at the crown and gradually widens. As time goes on, these two patterns can merge, creating the larger balding zones seen at the higher Norwood stages.
Understanding these patterns is important for two reasons. First, it helps set realistic expectations: if you’re thinning only at the temples in your early 30s, you may never progress beyond a moderate Norwood stage. On the other hand, if you see both temple recession and crown thinning before age 25, the chances of reaching more advanced stages are higher.
Second, it helps guide treatment. Early intervention can preserve existing hair, but once large areas are lost and scarred over, regrowth is much harder, if not impossible.
In other words, the Norwood scale isn’t just a chart—it’s a roadmap that shows where you are and gives clues about where you might be heading. The sooner you know your pattern, the sooner you can act to protect what you have.
The Role of Genetics and Metabolism
Genetics certainly set the stage for hair loss, but they don’t write the entire script. Your DNA determines how sensitive your follicles are to DHT and whether you’re predisposed to follow a particular balding pattern. That’s why two men of the same age and hormone levels can look completely different—one with a full head of hair, the other with advanced thinning.
But while you can’t change your genes, you can influence how those genes express themselves. One of the biggest external drivers of hair loss is metabolic health, particularly insulin resistance. When your body struggles to regulate blood sugar, levels of the enzyme 5-alpha-reductase rise, converting more testosterone into DHT.
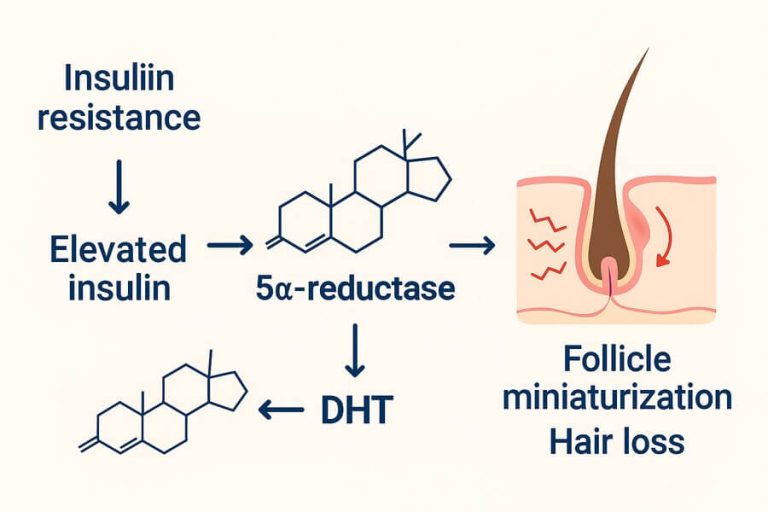
At the same time, the liver loses some of its ability to balance hormones, leaving more free testosterone available to be turned into DHT. This metabolic shift creates the perfect storm for accelerating follicle miniaturization.
The connection goes beyond hormones. Insulin resistance and poor metabolic health increase systemic inflammation and impair circulation, both of which damage the delicate environment around the follicle. Over time, this leads to the oxygen shortage, mitochondrial slowdown, and scarring that lock hairs in the “off” position.
This is why two people with the same genetic predisposition can have very different outcomes. One who maintains good metabolic health may keep most of their hair well into middle age, while another with poor diet, obesity, or chronic stress may lose it far more quickly.
In short, genetics load the gun, but metabolism often pulls the trigger. If you’re aiming to address your hair loss, you absolutely need to get your metabolism in order first by reducing insulin resistance.
For more information on metabolic health, I recommend reading up on my ketogenic diet article here. While I’m not necessarily suggesting this diet to fix your metabolic health, it does cover the topic of insulin resistance quite thoroughly.
Treatments for Hair Loss
Finasteride/Dutasteride
When it comes to medications for hair loss, few are as well-studied as finasteride and dutasteride. Both belong to a class of drugs called 5-alpha-reductase inhibitors (5-ARIs). They work by blocking the enzyme that converts testosterone into dihydrotestosterone (DHT), the hormone that miniaturizes hair follicles in androgenetic alopecia.
Finasteride was originally approved to treat benign prostatic hyperplasia (BPH) and later gained approval for male pattern hair loss. Dutasteride, on the other hand, is officially approved only for BPH, though it’s often prescribed off-label for hair loss because of its stronger DHT suppression.
Finasteride (often sold under the brand Propecia) selectively inhibits type II 5-alpha-reductase, lowering scalp DHT levels by about 60–70%. In large clinical trials, over 80% of men maintained or improved hair count after 2 years compared to steady loss in placebo groups. Long-term follow-ups have shown continued benefit at 5 and even 10 years of use.
Dutasteride (Avodart), by contrast, blocks both type I and type II enzymes, reducing scalp DHT by over 90%. Head-to-head comparisons suggest it may be more effective than finasteride, especially for crown and vertex areas. However, dutasteride is not FDA-approved for hair loss in most countries, and its stronger suppression can mean a higher risk of side effects.
Both finasteride and dutasteride are available only by prescription, but in practice, and in my experience, most doctors are willing to prescribe them for hair loss if you ask directly.
While finasteride and dutasteride are among the most effective tools for slowing or halting androgenetic alopecia, they are not without risks. Reported side effects include reduced libido, erectile dysfunction, and mood changes, though these occur in a small minority of users.
In 2025, the European Medicines Agency (EMA) added suicidal thoughts as a possible adverse effect with finasteride, reflecting ongoing concern about neuropsychiatric impact. Still, for the majority of men, these drugs are well tolerated.
The reason finasteride has been linked to mood changes isn’t entirely clear, but one likely explanation is its effect on neurosteroids in the brain. By blocking 5-alpha-reductase, finasteride lowers not only DHT but also compounds like allopregnanolone, which normally help regulate mood through calming GABA pathways.
Reduced levels may contribute to anxiety or depression in some men, while sexual side effects and psychosocial stress can add to the burden. Although most users tolerate the drug well, this possible mechanism explains why regulators flagged a potential neuropsychiatric risk.
I personally took 1.25 mg of finasteride (finasteride is often prescribed in 5mg tablets which you cut into quarters) daily for around three years, and it absolutely worked — it halted my hair loss completely after around 6 months of taking it.
Fortunately for me, there were no noticeable side effects. The challenge came from the commitment: I simply didn’t want to take a pill for the rest of my life. Once I stopped, the gains I had maintained slowly slipped away, confirming what the studies also show: when you discontinue finasteride, hair loss resumes.
If your priority is to hold onto hair as reliably as possible, 5-ARIs are unmatched in effectiveness. But they demand long-term commitment, because their benefits disappear when you stop. For those who are more risk averse and unwilling to stay on medication indefinitely (like me), alternative strategies — microneedling, low-level laser therapy, topical stimulants, lifestyle optimization, and eventually hair transplant — become the core of a drug-free plan, as we will see later.
Minoxidil

While finasteride and dutasteride work by lowering DHT, minoxidil takes a completely different approach. Originally developed as a blood pressure medication, it was approved for hair loss after patients and doctors noticed an unexpected side effect: new hair growth. Today, minoxidil, commonly sold under the (expensive) brand name Rogaine, is one of the most widely used and well-studied treatments for androgenetic alopecia.
Minoxidil works as a potassium channel opener, which relaxes blood vessels and improves blood flow to the scalp. This vasodilation increases the supply of oxygen and nutrients to hair follicles, but researchers believe its benefits go further: it also lengthens the anagen (growth) phase of the hair cycle and may directly stimulate follicular stem cells. In practical terms, this means hairs that were miniaturizing get more energy and time to thicken up again.
Clinical studies consistently show that topical minoxidil (2–5%) slows hair loss and promotes regrowth in both men and women, with visible improvement often appearing around 4 months and more significant gains by 6–12 months. In fact, a long-term follow-up study found that patients who stuck with minoxidil maintained benefits for many years, while those who stopped typically lost their gains within months. More recently, low-dose oral minoxidil has also emerged as an option prescribed off-label by dermatologists, often for patients who don’t respond well to topical treatment.
Minoxidil is the closest thing we have to a universal first-line therapy for hair loss. If you want to keep what you have and possibly regrow what you’ve lost, it’s almost always worth including in your regimen—especially when combined with microneedling or LLLT for an added boost.
Unlike finasteride, minoxidil can be bought from most grocery stores, often under the brand name Rogaine. Cheaper generic minoxidil also exists, typically as a 5% liquid or mousse (can sometimes be found in 2% which is preferable for some women). Costco often sells the 5% mousse, at around $50 for a 6-month supply.
Recently, low-dose oral minoxidil (0.25–5 mg/day) has gained popularity as some studies show it produces better results for those who don’t respond well to topical application. Both topical and oral minoxidil work through the same mechanism—improving blood flow and stimulating follicle activity—but they differ in delivery and strength.
Studies show both forms can promote regrowth and slow loss, but oral minoxidil tends to produce stronger, more consistent results—albeit with a slightly higher risk of side effects like water retention, body hair growth, and mild drops in blood pressure.
The main drawback is commitment: minoxidil is not a cure, and its effects last only as long as you continue using it. Some users also experience scalp irritation, itching, or unwanted hair growth on the face and body. Still, compared to most options, it’s relatively safe, affordable, and accessible without a prescription in most countries.
Many users also report that minoxidil also works best when combined with microneedling, which enhances absorption and further stimulates follicle stem cells for a synergistic effect.
Ketoconazole shampoo

Although ketoconazole started life as an antifungal medication, it has quietly earned a reputation as one of the best adjuncts for hair loss. Sold in 1% over-the-counter and 2% prescription strengths, ketoconazole shampoo helps maintain a healthy scalp environment—something that’s often overlooked in the fight against thinning hair.
Its primary role is to reduce inflammation and micro-organisms on the scalp. By controlling yeast such as Malassezia and lowering inflammatory cytokines, ketoconazole helps calm irritation that can worsen follicle stress. But research suggests it goes beyond hygiene: studies have shown that regular use of 2% ketoconazole shampoo can modestly reduce scalp DHT levels and improve hair density, acting as a mild topical anti-androgen. In another comparative trial, its performance was found to be similar to 2% minoxidil for maintaining hair thickness when used several times per week.
In practical terms, using ketoconazole shampoo two to three times per week can support whatever other treatments you’re using—whether that’s minoxidil, microneedling, or red-light therapy. It’s best to leave it on the scalp for about 3–5 minutes before rinsing to give the active ingredient time to work.
Ketoconazole isn’t a stand-alone cure for hair loss, but it’s one of the easiest, lowest-maintenance ways to improve scalp health, control inflammation, and enhance the effectiveness of stronger treatments.
Its effects are modest compared to finasteride, 5% minoxidil, or microneedling, and it can be a bit pricey over time—but if you’re aiming for maximum results or building a strong non-drug routine, ketoconazole shampoo is an excellent supporting player.
Platelet-Rich Plasma (PRP) Therapy

Platelet-Rich Plasma (PRP) therapy has become one of the most talked-about hair restoration techniques of the past decade—and for good reason. Unlike medications or topicals, PRP uses your own blood to stimulate dormant follicles and repair the scalp environment from within.
The process is simple in concept but sophisticated in effect. A small amount of your blood is drawn, then spun in a centrifuge to separate the plasma rich in growth factors and signaling molecules—including platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), and transforming growth factor beta (TGF-β).
These compounds are key to wound healing, angiogenesis (new blood vessel formation), and tissue regeneration. When injected back into thinning areas of the scalp, they help revive follicle stem cells, boost blood flow, and prolong the hair growth phase.
Clinical studies have shown encouraging results. Meta-analyses report significant increases in hair density and thickness after 3–6 monthly sessions, particularly when PRP is combined with minoxidil or microneedling. In one systematic review, over 80% of patients experienced visible improvement, with the best outcomes seen in early-to-moderate androgenetic alopecia. The procedure is generally safe since it uses your own plasma, though temporary redness or tenderness at the injection site is common.
PRP isn’t cheap—sessions typically cost several hundred dollars and need maintenance every 6–12 months—but it’s one of the most biologically compatible and evidence-backed non-surgical options available.
In practice, the results people see from PRP therapy are mixed. Some users describe it as an expensive disappointment with little to no new growth, while others claim it helped them recover a noticeably fuller head of hair. The truth likely lies somewhere in between.
PRP clearly has the potential to stimulate significant regrowth, but its success depends on many variables—factors like individual insulin sensitivity, overall metabolic health, the aggressiveness of your hair loss, and whether you’re combining it with other treatments such as finasteride, minoxidil, or microneedling.
If you haven’t addressed underlying issues like insulin resistance or chronic inflammation, PRP may not deliver strong results. On the other hand, if your loss is mild and you’re already supporting follicle health through other therapies and a healthy lifestyle, outcomes are usually much better.
Ultimately, the science isn’t yet advanced enough to predict who will respond and who won’t. We know it works very well for some, but not for everyone. As with much of hair restoration, trial and error still plays a role—and given PRP’s high cost, it’s often best viewed as a later-stage or “booster” option rather than the first thing to try.
Microneedling

Microneedling has quickly become one of the most effective non-drug treatments for hair loss — and one of the few with real scientific backing. Originally used in dermatology for scar reduction and skin rejuvenation, the technique involves using fine needles to create controlled micro-injuries in the scalp. These tiny punctures trigger the body’s natural healing response, which releases growth factors, improves blood circulation, and stimulates stem cells in the hair follicle bulge— the very cells responsible for new hair growth.
We now have several studies that confirm its benefits. In a landmark randomized trial, men who combined weekly microneedling with 5% minoxidil showed over four times more new hair growth than those using minoxidil alone. More recent reviews and meta-analyses support these results, consistently showing that microneedling enhances the absorption and effectiveness of topical treatments while independently stimulating follicular regeneration.
The key variable is needle depth.
- 0.25–0.5 mm: Primarily improves topical absorption (great for combining with minoxidil or caffeine serums).
- 1.0–1.5 mm: Reaches the level of follicular stem cells, ideal for true regenerative stimulation.
- >1.5 mm: No added benefit, with higher risk of irritation or scarring.
At-home microneedling kits — such as derma rollers or motorized pens — can be highly effective when used correctly. While recent FDA changes have made motorized devices harder to purchase for home use, they are still available.
I personally use the Dr. Pen M8S, set to 1.0 mm once per week, which is typical for scalp application. Cleanliness is crucial: always sterilize the device before and after with isopropyl alcohol, and never use it on inflamed, infected, or actively shedding skin. Mild redness for 12–24 hours is normal, but avoid applying minoxidil immediately afterward — waiting a full day helps prevent irritation.

Microneedling can also be performed professionally. Dermatologists use medical-grade pens with precise depth control and sterile, single-use cartridges, though costs are naturally higher — typically $400–$500 per session.
For those like myself experiencing slow, steady thinning, microneedling combined with topical minoxidil (and a healthy metabolic profile) can significantly slow hair loss progression. It requires consistency and patience, and results may decline as DHT levels rise with age — but for early or mild cases, it remains one of the most effective drug-free strategies available.
LLLT and Red Light Therapy

Light therapy for hair growth might sound futuristic, but it’s one of the most scientifically supported non-drug treatments available. The technical term is Low-Level Laser Therapy (LLLT) — sometimes called red light therapy — which uses specific wavelengths of red (around 650 nm) and near-infrared light (up to 850 nm) to stimulate hair follicles.
While “red light” and “LLLT” are often used interchangeably, LLLT usually refers to medical-grade laser or LED devices that deliver light at a higher and more consistent power output. The goal is to energize the follicle’s mitochondria — the cell’s powerhouses — which boosts ATP production, oxygen utilization, and local circulation. This helps reactivate sluggish follicles, extend the anagen (growth) phase, and reduce scalp inflammation.
Clinical evidence is strong. In a 16-week randomized, double-blind trial, men using a 655 nm helmet device every other day saw about a 35% increase in hair counts versus placebo.
Multiple reviews/meta-analyses have since confirmed LLLT improves hair count and thickness with minimal side effects.
However, not all devices are created equal. Many inexpensive “red light masks” and handheld panels emit too little power to penetrate deeply enough to reach the follicles. Studies showing positive results typically used power densities of 50–100 mW/cm², delivered for 10–20 minutes, several times per week.
This is why FDA-cleared laser caps and combs (like Capillus, iRestore Professional, or Kiierr 272) tend to outperform cheap consumer devices — they simply deliver enough energy to trigger biological change.
From my research and speaking with those who use them (and who have seen improvements) the market leaders seem to be iRestore, Hairmax, and theradome. These can get costly, however, with top-of-the-range models costly between $1,000 to $2,000 dollars. Unfortunately, it seems you would be better off not buying anything than buying a cheap one.

Results are gradual but real, especially when combined with treatments like microneedling or minoxidil. In fact, it is likely the most powerful drug-free trio available right now. Just make sure your device is powerful enough to make a difference — most aren’t. It is also imperative that you do some thorough research when looking for a cap, as there are lots of dubious claims from various companies. Reddit or other forums will be your friend here.
Topical Caffeine & Rosemary Oil
For those who prefer a natural or drug-free approach — or who don’t respond well to minoxidil — there are a few promising topical options that have begun to attract serious scientific interest. Among them, topical caffeine and rosemary oil stand out as the best-supported alternatives.
Caffeine doesn’t just wake up your brain — it can wake up your hair follicles, too. In laboratory studies, topical caffeine has been shown to counteract DHT’s suppressive effects on follicle cells and stimulate cell proliferation within the hair bulb.
A 2018 clinical study comparing 0.2% caffeine solution to 5% minoxidil found the two produced comparable improvements in hair density after six months, though larger trials are still needed to confirm these results. Caffeine also boosts scalp microcirculation and may extend the anagen (growth) phase of the hair cycle.
In practice, caffeine works best as a daily leave-in tonic or serum, ideally left on the scalp for several hours rather than rinsed out quickly like a shampoo. It’s a mild, well-tolerated compound with virtually no systemic side effects — making it a smart addition for those seeking a low-risk, supportive option.
And for those wondering, no, drinking coffee or energy drinks will not have the same effect. It must be topically applied.
Rosemary oil is another natural treatment that’s shown surprising scientific merit. In a 2015 randomized trial, participants applying rosemary oil twice daily saw similar hair growth to 2% minoxidil after six months — with fewer reports of scalp itching or irritation.
Rosemary contains compounds such as carnosic acid and rosmarinic acid, which may improve blood flow, reduce inflammation, and protect follicle mitochondria from oxidative stress.
To use it safely, dilute 1–2% rosemary essential oil (about 6–12 drops per 30 mL of carrier oil such as jojoba or argan) and massage it into the scalp 3–5 times per week. It can also be layered with microneedling or red-light therapy to enhance penetration and cellular activation.
While neither caffeine nor rosemary oil can yet match the robust data supporting minoxidil or finasteride, both offer real, biologically plausible benefits — especially when combined with mechanical or light-based stimulation. For anyone seeking a gentler, more natural routine, they represent the best evidence-backed options available today.
Nutrients That Support Hair Growth
Even the best treatments—whether topical or mechanical—can’t compensate for missing raw materials. Hair is made primarily of keratin, a protein that depends on a constant supply of amino acids, minerals, and vitamins to grow. When the body is undernourished or metabolically imbalanced, it prioritizes vital organs over hair, which is why nutritional deficiencies often show up first as thinning or shedding.
Among the most important nutrients are vitamin D, zinc, iron, and B-vitamins, all of which play direct roles in follicle health and regeneration. Vitamin D helps regulate the hair growth cycle and activate dormant follicles, while zinc supports cell division and reduces inflammation around the follicle bulb.
Iron—especially the heme form found in red meat and liver—is essential for oxygen delivery to the follicle’s mitochondria. Low ferritin (iron storage) is strongly correlated with telogen effluvium and chronic shedding. Biotin is another commonly cited nutrient; while true biotin deficiency is rare, it contributes to keratin production and is sometimes beneficial in those with brittle or slow-growing hair.
A high-protein, nutrient-dense diet naturally rich in these micronutrients tends to outperform supplementation alone. Foods like liver, eggs, oysters, sardines, beef, and fermented vegetables offer the right balance of iron, zinc, selenium, and vitamin C—all crucial for collagen and connective tissue formation around the follicle. Vitamin C, in particular, enhances iron absorption and supports antioxidant defenses in the scalp environment.
Once again, metabolic health matters greatly. Insulin resistance not only drives DHT conversion but also impairs nutrient delivery to hair follicles by stiffening blood vessels and raising inflammation. Optimizing blood sugar through low-carbohydrate or nutrient-dense whole-food diets may indirectly support healthier, thicker hair over time.
Final Thoughts
Hair loss isn’t caused by just one factor. While genetics set the stage, it’s ultimately driven by a mix of hormonal imbalance, inflammation, oxygen deprivation, and mitochondrial decline within the follicle — processes that are heavily influenced by metabolic health and lifestyle.
The most effective approach therefore isn’t a single product or pill, but a multi-layered strategy that supports the entire follicle ecosystem: improving circulation and oxygenation with microneedling or red-light therapy, reducing DHT’s impact through finasteride or dutasteride, and strengthening the body from within with nutrient-dense foods and balanced insulin levels.
It’s worth being clear: for most people with androgenetic alopecia, 5-alpha-reductase inhibitors like finasteride and dutasteride remain the only consistently proven way to halt hair loss long-term. They address the hormonal root cause — DHT — which no other treatment can fully block. However, taking medication indefinitely is a personal decision.
While long-term safety data are largely reassuring, many (myself included) prefer not to commit to a lifelong drug regimen. In that case, natural or mechanical options — microneedling, red-light therapy, caffeine, rosemary oil, or ketoconazole shampoo — can still offer meaningful results, though typically to a lesser degree since they don’t neutralize DHT directly.
The key is understanding your priorities and physiology. If you’re comfortable with medication, finasteride or dutasteride offer the strongest defense. If not, you can still build a powerful, holistic routine by optimizing scalp health, improving mitochondrial energy, and supporting metabolic balance.
FAQs
What is the best treatment for hair loss?
It’s worth being clear: for most people with androgenetic alopecia, 5-alpha-reductase inhibitors like finasteride and dutasteride remain the only consistently proven way to halt hair loss long-term. They address the hormonal root cause — DHT — which no other treatment can fully block. However, taking medication indefinitely is a personal decision.
How do I stop my hair from falling out?
The most effective approach therefore isn’t a single product or pill, but a multi-layered strategy that supports the entire follicle ecosystem: improving circulation and oxygenation with microneedling or red-light therapy, reducing DHT’s impact through finasteride or dutasteride, and strengthening the body from within with nutrient-dense foods and balanced insulin levels.
What is the main cause of hair loss?
Hair loss isn’t caused by just one factor. While genetics set the stage, it’s ultimately driven by a mix of hormonal imbalance, inflammation, oxygen deprivation, and mitochondrial decline within the follicle — processes that are heavily influenced by metabolic health and lifestyle.